There are two main types of bone marrow transplants discussed in the literature, autologous and allogeneic. Autologous transplants are performed by using the patient’s own stem cells, collected from the bone marrow, and then reinjected back into the patient. This is done because chemotherapy/radiation therapy can kill bone marrow and blood-producing cells. Allogenic transplants, on the other hand, use cells from a donor rather than preserving and administering the patient’s own cells after a procedure. One benefit of using this method is the graft-versus-tumor effect, which is when the donor’s T cells attack the patient’s tumor.
As mentioned previously, the first part of this process is where stem cells are collected from the blood or bone marrow, depending on the patient’s current health status. To prep the patient for this procedure, the patient then undergoes chemotherapy/ radiation therapy. This preparation will not only damage/ destroy the disease, but it also acts to pacify the immune system so that the later transplant is not rejected by the body. Next, cells, whether they are from a donor or the patient themselves, are injected into the bloodstream. From here, cells travel to the bone marrow, where they attach to other cells and begin to reproduce the cells lost during the chemotherapy treatment.
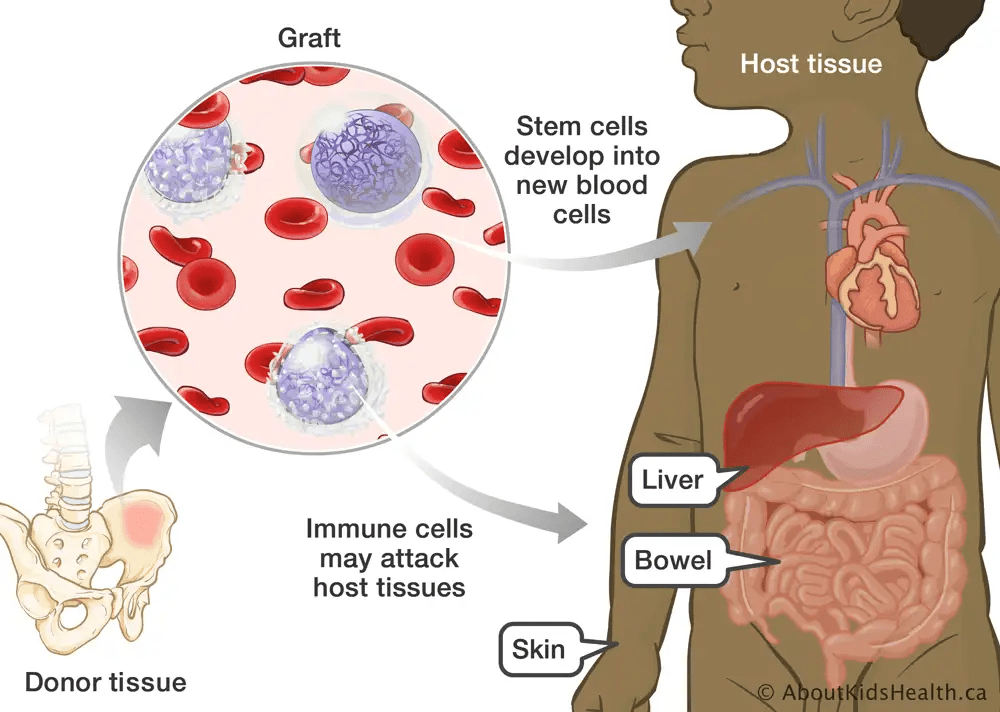
Image created by AboutKidsHealth.ca
A match is considered to be 10/10 if the donor and recipient have identical alleles present at all 5 HLA (human leukocyte antigen) loci. If the donor and recipient are not 10/10 matches, then the chance of complications rises; one example of this is graft-versus-host-disease (GVHD), where the grafted cells attack the patient’s body. You are most likely to find a 10/10 match by looking to a patient’s siblings (specifically full siblings). If this is not possible, then the most valuable resource for finding a match is the donor registry, where many different doses are preserved in case a future patient can not find a match through normal methods. Because of this, it is important for as many people as possible to donate, as it increases the likelihood of a match being found for patients with no families.
A haploidentical match occurs when a donor only matches half of the patient’s HLA alleles. This means that these types of matches only share 1 haplotype, which is where the name originates. This match is less preferable than the 10/10 match, but the advantage is that it is much easier to find this match type among the patient’s family as well as in the donor registry. This match is always found in the form of parents and children of the patient, but also with siblings at a lower rate. In the past, haploidentical matches showed a much higher complication rate, but with the use of modern technology, the chances of these events occurring are much lower.
GVHD is a common complication for patients undergoing a bone marrow transplant procedure. It occurs when a stem cell transplant attacks the host’s tissues rather than taking root properly. Specifically, it is the donor’s T lymphocytes that become activated when they contact the host cells’ antigens presented by HLA molecules. This can cause complications if the patient is not a 10/10 match with the donor, as the donor cells may recognize these molecules as invasive pathogens and attack them. This can occur in both types of bone marrow transplants, but it is more commonly seen in allogeneic transplants. In cases of severe GVHD, patients may experience both acute and chronic symptoms. Acute symptoms include rash, jaundice, vomiting, and diarrhea. Some chronic symptoms are scarring around the affected area, dry glands, muscle aches, organ damage, and possibly death.
The more HLA mismatches that are present between a donor and patient, the more likely the chances of negative outcomes. This is because it provides the donors’ T lymphocytes more chances to encounter mismatched HLA cells and attack them as foreign pathogens. Several treatments have been developed for GVHD; these include medications like corticosteroids and general monitoring and treatment of symptoms as they arise. The most effective treatment for treating GVHD, however, is still prevention. This is done by suppressing the immune response with various medications while still in the conditioning phase of a bone marrow transplant.